The population, intervention, comparator, and outcomes (PICO) element of the upcoming EU Joint Clinical Assessment (JCA) is an area associated with high uncertainty and anticipation amongst manufacturers. The recent publication of six PICO exercises (three medicinal products [MPs], three medical devices [MDs]) by the Member State Coordination Group on Health Technology Assessment (HTA CG) offers valuable insights into expected evidence requirements for manufacturers (Table 1).1-6
| Technology | Indication | # PICOs |
|---|---|---|
| Durvalumab | Advanced or unresectable hepatocellular carcinoma | 13 |
| EASEE system | Focal onset epilepsy | 5 |
| Adagrasib | Advanced non-small cell lung cancer (NSCLC) with KRAS G12C mutation | 13 |
| Edwards EVOQUE Tricuspid Valve Replacement System | Severe tricuspid regurgitation | 1 |
| Etranacogene dezaparvovec | Haemophilia B (congenital Factor IX deficiency) | 7 |
| PDA stenting with a bioabsorbable stent | Neonates and infants with cyanotic congenital heart defects | 3 |
The HTA CG has emphasised that these exercises were used to test and refine the scoping process and therefore do not reflect the final endorsed guidance. Notably, these exercises were conducted on MPs that had already received positive opinions from the European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP), and MDs that had received scientific opinions from expert panels.7 In practice, manufacturers would not have access to these opinions at the time of the JCA. Despite these caveats, these exercises offer a clearer understanding of the rationale behind PICO consolidation, helping manufacturers refine their approach to JCA evidence generation.
Dissecting the PICO
Population
A key takeaway from these exercises is the role of sub-populations in reflecting varying clinical practices across member states. This is particularly relevant for oncology medicinal products (i.e., adagrasib and durvalumab), where the number of populations was highest (Figure 1).
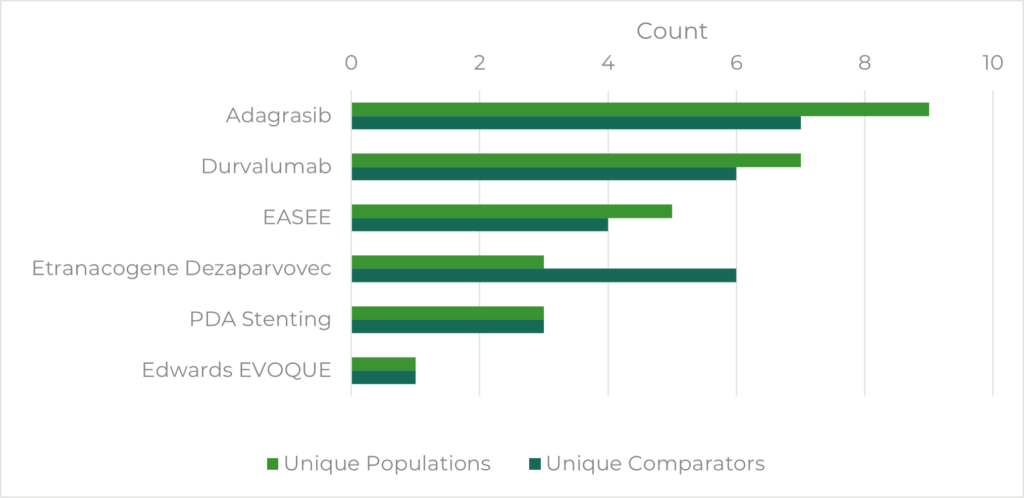
For adagrasib, nine separate populations were identified, with eight sub-populations according to3:
- Line of therapy
- Treatment sequence (e.g., immune checkpoint inhibitors first vs chemotherapy first)
- Histology variations (adenocarcinoma vs squamous NSCLC)
The large number of populations significantly impacted the final number of consolidated PICOs, as each distinct sub-population requires its own dedicated PICO, markedly increasing the complexity and volume of data required of manufacturers.8 This highlights the importance of anticipating all possible population variations at an early stage, ensuring the evidence package adequately captures the comprehensive data requirements of each sub-population.
It is also important to note that sub-group analyses do not necessitate an entirely separate PICO. For example, in PICO exercise 4, the JCA sub-group requested an additional analysis within the existing population, comparing high versus intermediate surgical risk, rather than defining a separate one. This reinforces that sub-group analyses are conducted within a given PICO rather than requiring a separate one.4 When defining populations, manufacturers should consider whether additional groups might be classified as sub-groups (i.e., post-hoc analyses of treatment effects within patient subsets) or as sub-populations (i.e., requiring a separate PICO due to differences in the treatment approach).
Intervention
Given the parallel timelines between the EMA and JCA processes, the JCA dossier submission is scheduled to occur before the Summary of Product Characteristics (SmPC) label decision.9 Therefore, it is uncertain what the authorised indication will be, especially if the CHMP recommends a label that differs from the submitted one. The manufacturer may need to submit an updated JCA dossier, with deadlines ranging from 7 to 30 days, depending on the nature of the change.9 Manufacturers must, therefore, be adaptable and proactive, potentially preparing additional evidence scenarios in advance to quickly respond to label changes.
Comparator
As expected, differences in comparators reflecting the standard of care in member states resulted in a high number of PICOs during these exercises. This was especially evident for oncology MPs, where multiple populations often require different comparators or there may be a comparator that is only used in a particular patient sub-population.1,3 The PICO consolidation process aims to mitigate this complexity by incorporating ‘OR’ statements, allowing multiple comparators within a single PICO, as demonstrated in adagrasib (PICO exercise 3; Table 2).
| P | Adults with advanced non-small cell lung cancer (NSCLC) with KRAS G12C mutation after first-line treatment with cytotoxic chemotherapy – Sub-population |
| I | Adagrasib monotherapy |
| C | Docetaxel (only for patients with PD-L1 negative tumours), OR Pemetrexed (only for patients with PD-L1 negative tumours except in the case of predominantly squamous histology), OR Nivolumab, OR Pembrolizumab (only for patients with PD-L1 expressing tumours (TPS ≥1%)), or Atezolizumab, OR Docetaxel in combination with nintedanib (only for patients with PD-L1 negative tumours and adenocarcinoma histology) |
| O | See outcomes list |
Whilst comparator consolidation helps streamline the PICO process, manufacturers must still provide robust evidence for each comparator included in a consolidated PICO. Manufacturers should, therefore, identify and anticipate requests for unique comparators that, while potentially relevant to only a small number of member states, may still necessitate the creation of a separate PICO. In instances where no data is available – including for specific comparators – manufacturers may provide justification for a gap in evidence.8 The assessor and co-assessor will evaluate whether the justification is appropriate, and the final acceptability of the gap will be determined at the national level.8 To note, while missing data does not automatically invalidate the JCA, it does introduce uncertainty, and the threshold for what is deemed an adequate justification remains unclear.
Outcomes
A key result of the PICO exercises is the consolidation of outcomes across PICOs. The decision to create a single list of outcomes per technology supports a more efficient JCA process for stakeholders. However, this approach carries the risk of excluding certain clinically relevant outcomes, potentially overlooking more nuanced patient benefits. Additionally, despite consolidation, the number of outcomes remains substantial. For example, 14 outcomes were included in the consolidated outcomes list for the adagrasib exercise.3
A key challenge in this approach is ensuring that all necessary outcomes are available for comparators, particularly when ITCs are required. For instance, in the case of adagrasib, obtaining data on certain outcomes for every specified comparator may not be feasible. Since the consolidated outcomes are not ranked, manufacturers may be required to provide evidence for all listed outcomes across all comparators, regardless of data availability.
To mitigate these challenges, manufacturers should aim to align the outcomes collected in clinical trials with the likely outcomes list for JCA as closely as possible, to avoid data gaps and reduce the need for additional evidence generation.
Conclusion and Impact
Overall, the PICO exercises conducted by the HTA CG provide valuable insights into the evidence-generation requirements for the JCA. While early concerns regarding the potential complexity and volume of PICOs required for JCA are valid, these exercises demonstrate that the HTA CG has adopted a pragmatic approach to the selection process. This approach reduces the overall data burden while maintaining sufficient detail to satisfy member state requirements. However, the PICO process will continue to represent a significant investment for manufacturers, particularly for those lacking capacity in areas such as HEOR and statistics. Nevertheless, there are proactive strategies that manufacturers can take to mitigate the burden and impact of JCA evidence requirements:
- Early payer research/stakeholder engagement – Initiate early dialogue with clinical experts, payers, and patient stakeholders to understand the future PICO landscape and refine the trial design. If possible, engage with the HTA CG through JSC to provide more granular detail on what is to be expected from the outputs of the PICO scoping exercise
- Optimise evidence generation strategy – Incorporate early market insights into the Phase III trial design to ensure alignment with JCA PICO requirements
- Leverage real-world evidence (RWE) capabilities – Employ RWE techniques, such as indirect treatment comparisons and external control arms to address and fill evidence gaps, particularly where there is limited data on comparators. Where evidence gaps persist, prepare robust justifications for non-inclusion
- Optimise trial design – Adopt flexible, adaptive trial designs – such as incorporating multiple comparator arms or considering post-hoc subgroup analyses – to ensure the generated evidence can respond effectively to evolving JCA requirements
For further information on how to start planning and implementing changes immediately in preparation for EU HTA, watch our webinar on taking action.
For more tailored help, get in touch to see how Remap can help develop materials for JSC and JCA or with bespoke training.
Citations and Reference List
- Member State Coordination Group on Health Technology Assessment. PICO Exercise MP 01: Durvalumab (Imfinzi®) for Adults With Advanced or Unresectable Hepatocellular Carcinoma (HCC) [published online Spring 2024]. Available from: https://health.ec.europa.eu/document/download/322ae969-f3ca-4f23-ab8e-1b4bdf22528f_en?filename=hta_pico_mp01_en_0.pdf. Accessed February 24, 2025.
- Member State Coordination Group on Health Technology Assessment. PICO Exercise MD 02: EASEE SYSTEM for Adults With Focal Epilepsy Refractory to Two or More Antiepileptic Medications [published online Spring 2024]. Available from: https://health.ec.europa.eu/document/download/4aacd064-8276-4b12-8c33-7979b67d378d_en?filename=hta_pico_md02_en.pdf. Accessed February 24, 2025.
- Member State Coordination Group on Health Technology Assessment. PICO Exercise MP 03: Adagrasib (Krazati®) for Adult Patients With Advanced Non-Small Cell Lung Cancer (NSCLC) With KRAS G12C Mutation After Disease Progression Following Prior Systemic Therapy [published online Spring 2024]. Available from: https://health.ec.europa.eu/document/download/63868893-b079-4ea6-bf94-af2cd9f19c65_en?filename=hta_pico_mp03_en_0.pdf. Accessed February 24, 2025
- Member State Coordination Group on Health Technology Assessment. PICO Exercise MD 04: Edwards EVOQUE Tricuspid Valve Replacement System for Patients with Severe Tricuspid Regurgitation [published online Spring 2024]. Available from: https://health.ec.europa.eu/document/download/288f7898-fbcd-4e64-b7be-70b6b38006bc_en?filename=hta_pico_md04_en.pdf. Accessed February 24, 2025
- Member State Coordination Group on Health Technology Assessment. PICO Exercise MP 05: Etranacogene dezaparvovec (Hemgenix®) for Adult Patients with Severe and Moderately Severe Haemophilia B [published online Spring 2024]. Available from: https://health.ec.europa.eu/document/download/dcaede60-e13c-45d2-9e1d-f2257ba81444_en?filename=hta_pico_mp05_en_0.pdf. Accessed February 24, 2025
- Member State Coordination Group on Health Technology Assessment. PICO Exercise MD 06: PDA Stenting with a Bioresorbable Stent in Neonates and Infants with Cyanotic Congenital Heart Defects [published online Spring 2024]. Available from: https://health.ec.europa.eu/document/download/c62fd888-631f-4a0b-8764-cc5f5706ddc5_en?filename=hta_pico_md_6_en.pdf. Accessed February 24, 2025
- Member State Coordination Group on Health Technology Assessment. Cover Letter for PICO Exercises on Medicinal Products (MPs) and Medical Devices (MDs) [published online Spring 2024]. Available from: https://health.ec.europa.eu/document/download/8a53f67a-8593-4acc-9b24-c0faab913a86_en?filename=hta_pico_cover_en.pdf. Accessed February 24, 2025
- Member State Coordination Group on Health Technology Assessment. Guidance on the Scoping Process. Version 1.0. Adopted November 28, 2024. Available from: https://health.ec.europa.eu/document/download/7be11d76-9a78-426c-8e32-79d30a115a64_en?filename=hta_jca_scoping-process_en.pdf&prefLang=de. Accessed February 24, 2025
- Member State Coordination Group on Health Technology Assessment. Procedural Guidance for Joint Clinical Assessments of Medicinal Products. Version 1.0. Adopted November 28, 2024. Available from: https://health.ec.europa.eu/document/download/0929cd01-619d-4456-a1c4-d8e33f9e36bf_en?filename=hta_jca_mp_procedural-guidance_en.pdf. Accessed February 24, 2025.